I have a button-hole fistula, I had the fistula surgery in 2009 and began using it after about three months. I used it with no issues over the next year while I dialyzed in-center three time per week.
I began research into home hemodialysis using the NxStage System One, and decided I would prefer to use home hemo instead of in-center hemo. I also decided I would need a button-hole fistula to easily allow me to insert my own needles for home hemo.
My button-hole fistula was created by a Master Phlebotomist. Sharp needles are carefully placed for the best blood flow, then I dialyzed like normal. The same Phlebotomist inserts the sharp needles in the same holes she initially created each time I dialyzed for about 12 to 15 more times. This forms scar tissue to allow the use of dull fistula needles.
This also allows my fistula to last longer, sharp needles cause damage to the skin over the fistula and to the fistula. My button-hole fistula will allow it to last longer, provide me with much easier methodology for needle insertion, and for me, dull needles are MUCH less painful than sharp needles.
Three days ago I had my fistula checked by an arterial surgeon. After over four years of use I was having trouble placing my arterial needle. I was sure I didn’t have a clot, but couldn’t seem to find the proper track to insert the needle.
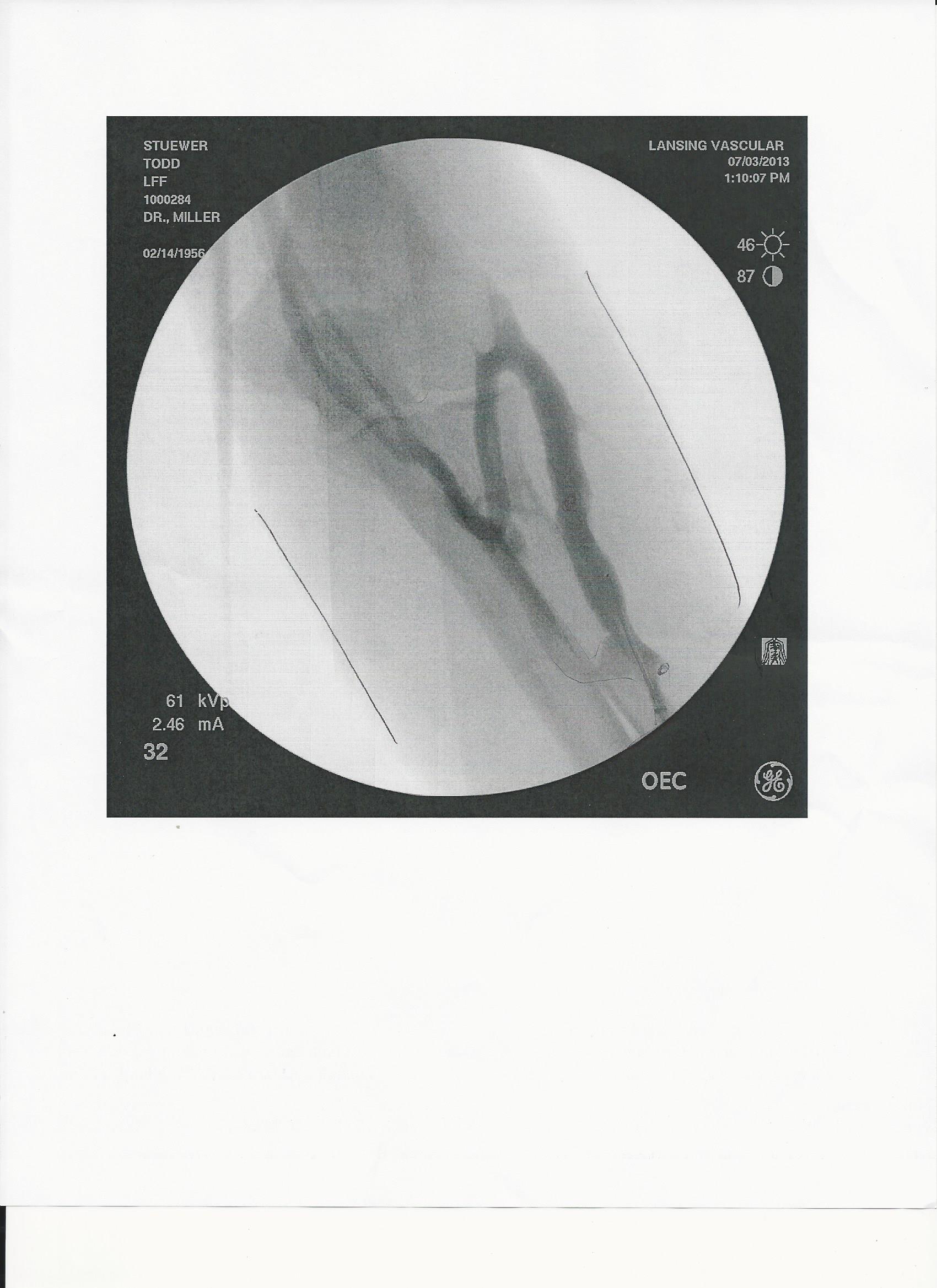
I called my dialysis nurse to discuss the problem I was having and she asked me to come in to check my fistula. She listened to it with a stethoscope and it sounded normal. She had me hold a needle and demonstrate the angle I used to insert the needle, and my “turn” (I have an unusual fistula that quires me to insert the needle about halfway, then perform about a 45 degree turn, before continuing the full insertion of the needle (See picture of my fistula from the arterial surgeon below).

She felt that I was not getting the proper final angle to complete the needle insertion. That night I used the angle she suggested and got the needle in much more easily. And, like usual, I ran at my normal run speed of 500.
She asked me when I last had my fistula checked by an arterial surgeon. I replied that I had not seen one since I had a clot removed in the venous portion of my fistula over 18 months ago. She was surprised and said I should have it reviewed periodically and made an appointment with the vascular center.
The arterial surgeon did an ultra-sound of my fistula, compared it to the photo taken during my prior visit, discussed the issues I was having and determined that my fistula was in great shape.
He described that button hold fistulas have a flap of skin at the end of the scar tissue, and that the flap had to be moved out of the way while inserting the dull needle, and that scar tissue changes over time. I was simply having some problems accounting for the changes in scar tissue. After reviewing the photo of my fistula with him, I am right back to easily inserting the needle.
He also told me I should have my fistula checked every six months to verify it is working properly, and to prevent having problems in the future. I now have my next review appointment scheduled.
He also provided me with the following important information about the three conditions for fistulas:
Green – All Clear – Everything is normal, keep up the good work
Normal thrill (vibration)
Blood flow rates normal
Venous pressures normal
Arterial pressures normal
Bleeding less than 15 minutes after dialysis
No problems getting needles in
No pain, redness or swelling
Clearance labs normal
Yellow – Caution – Ask dialysis nurse for referral to vascular center
Thrill (vibration) weaker
Hard to get needles in
Frequent alarms on machine
Bleeding more than 15 minutes after dialysis
Pulling clots during needle insertion
Inadequate dialysis (clearance)
Low blood rates
Cold or painful hand during dialysis
Arm or hand swelling
Red Zone – Access emergency – Contact vascular center immediately
Clotted access (no thrill/vibration)
Can’t put needles in
Broken or clotted catheter
Drainage at needle sites or incision
Signs of infection:
- Redness
- Swelling
- Pain
- Skin warm to the touch
It’s pretty simple to avoid any of these problems by simply having it checked periodically by an arterial surgeon.